- ホーム
- 歯の矯正(大阪/吹田)
- Considering whether orthodontic treatment is necessary (adult orthodontics)
Considering whether orthodontic treatment is necessary (adult orthodontics)blog
When forming treatment plans, there is often discussion about whether a patient needs orthodontic treatment.
Here I have collected my own thoughts about full-jaw treatment in particular on deciding if to perform orthodontic treatment.
Please share this if you think it is useful.

I am a general practitioner. I have a neutral view of treatment since I am not a specialist, so I hope this will serve as a reference.
Orthodontics is widely divided into two fields.
1. Occlusal guidance during childhood ・・・There will still be growth of the upper and lower jaw. Occlusal guidance is very important early in this stage.
2. Adult treatment ・・・Growth of the upper and lower jaw is unlikely. There is a low ability to adapt, and acclimation (attrition) with enamel is not likely with a prosthesis. The difficultly increases with complex conditions such as cavities, periodontitis, and tooth loss.
Here we will focus on whether to do adult treatment. (Children do not come to my clinic) There are common purposes between both child and adult treatment, but it can be confusing if talked about at the same time.
For purposes here, we will have to think about any risks with treatment.
When talking about getting treatment, because most people’s teeth has some sort of problem, if a perfect alignment is the standard, then everyone would need treatment.
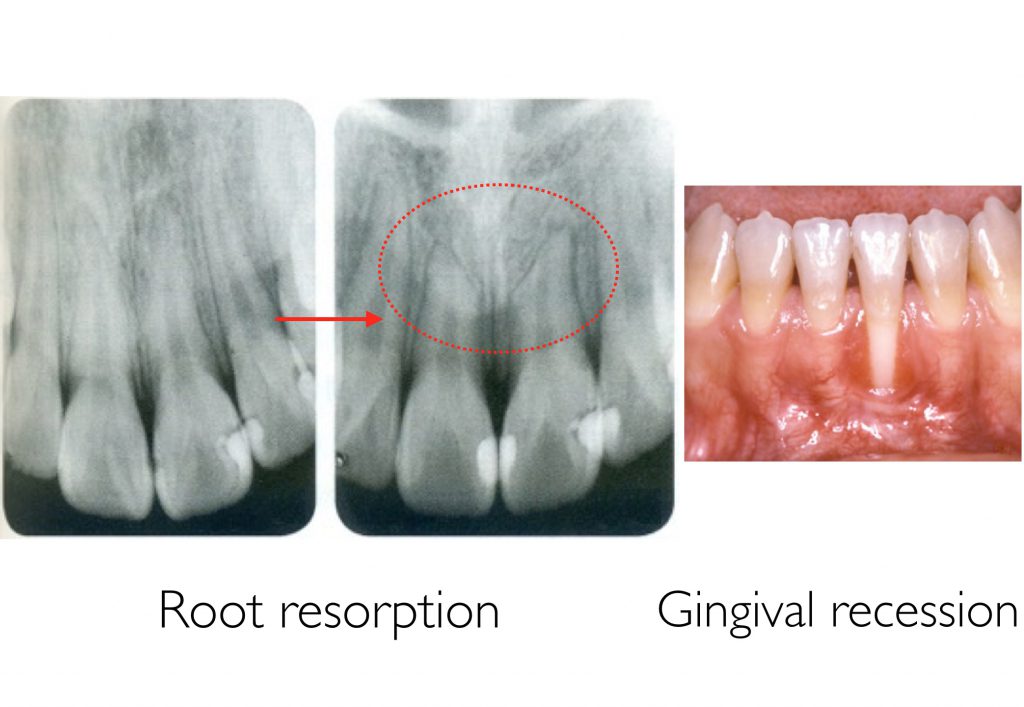
However, treatment is accompanied by things like a time frame, money, retrogression, pain, and complications. There is a risk of root resorption, gingival recession, and other complications. That is why it is necessary to think about the need for treatment while considering these risks.
There are many orthodontists who themselves do not get treatment if their teeth are misaligned.
They know that treatment will make their teeth look better, but after thinking about the cost, time frame, pain, retrogression, complications and other risks, they decided themselves whether to have treatment even as orthodontists.
In adult orthodontics, these are the 5 reasons to perform treatment.
1. To improve appearance
2. To improve cleaning
3. To improve eating and chewing
4. To prevent tooth loss due to force
5. Other (per opportunity)
There are many reasons it would be best to perform treatment. I think about the necessity of treatment by comprehensively thinking about all of them. On the other hand, a comprehensive decision in the end would become confusing and mix the issues together. To avoid this, I first categorize the problems. In addition, because there are bound to be multiple problems, I will finally make a decision as a whole.
First is
1. Appearance
Although this is the easiest to grasp, there are a lot of people who do not have a clear understanding.
To begin with, appearance is decided by how the patient feels. Therefore, I think it would be a little strange for an orthodontist to arbitrarily discuss the need for treatment. But because we are professionals, I also think we should make suggestions. For example, if orthodontic treatment would benefit the patient, how different they are numerically from the average person, and what kind of goals they could achieve with treatment with time and money. Even so, the decision is made by the patients themselves.

Most patients come to orthodontists with appearance in mind.
Conversely, general practitioners tend to overlook this important part.
Appearance is broken into two parts: facial, and intraoral.
Facial appearanceis divided into the following:
– Maxillary protrusion (overbite)
– Bimaxillary protrusion (double protrusion)
– Mandibular protrusion (underbite)
Often only intraoral photographs are observed to discuss the need for treatment.
Many general practitioners think about treatment especially in terms of preserving the teeth, and I see cases where there are no photographs that show the facial appearance (particularly from the side) even when consulting patients.

A photograph showing the face is invaluable when discussing whether there should be orthodontic treatment.
For example,

when patients like in the picture above visit, it is not possible to discuss during their examination about the need for orthodontic treatment using only an intraoral photograph.
The appearance is good, the vertical stop (intercuspal position) is stable, and the anterior guidance (molar disclusion) is excellent.
However, if you can see an overbite from the side, you can suggest treatment to improve the appearance.


Although it is sometimes possible to estimate the facial appearance with tooth angles from inside the mouth, it is clear that the appearance is necessary to make a diagnosis.
By the way, the appearance of overbites cannot be improved with tooth straightening alone. If the patient would like their facial appearance to be improved by retracting their lower jaw, orthognathic surgery (osteotomy) is required. (A cephalometric analysis is used to determine the possibility of tooth straightening)

Intraoral appearance
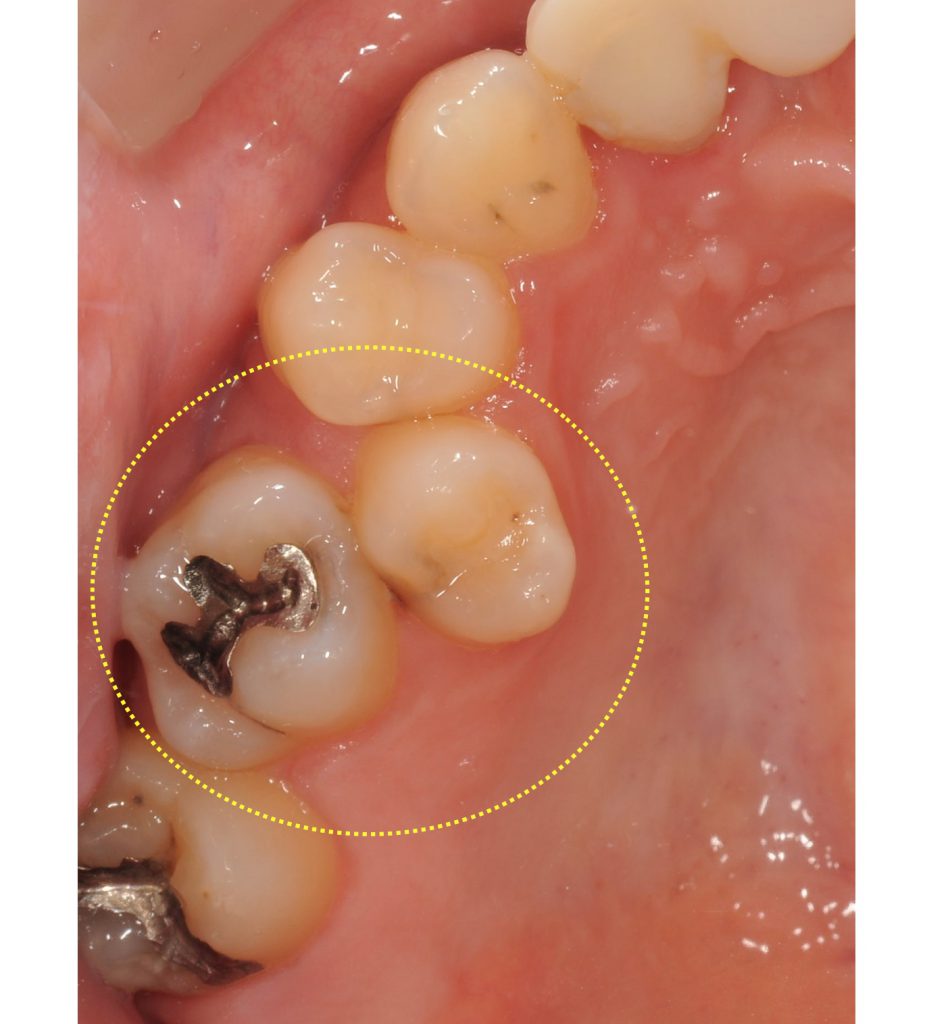
If a patient like in the picture below visits, their facial appearance is perfect.

Nevertheless, you can see a lot of crowding once you look inside their mouth. You must confirm if this bothers the patient.

Think about whether to perform orthodontic treatment to improve appearance while considering these examples.
2. Cleanability


It is common to hear the general public say that it is better to get orthodontic surgery if you have crowded teeth (misalignment) since it is harder to brush them and causes cavities and periodontitis.
It is not a strange thing to recommend treatment to patients with crowding.
But it should also be kept in mind that if they can properly clean their teeth even with crowding, then there is no need for treatment. It is too quick to think about treatment to improve cleanability just from looking intraorally and seeing crowding and built-up plaque.
First, instruct them on proper brushing and flossing techniques. Then, if there are still no improvements, treatment can be recommended.

Of course, cleanability will increase with better alignment if there is crowding, so treatment would be better.
Treatment comes with risks such as cost, time frame, complications, and retrogression, so it becomes necessary to have a basis to recommend treatment as a professional. Certainly, if patients want better tooth alignment with appearance, it would be better to get treatment.
Cleanability may increase with treatment, but you should know if there is a basis to do so.
Would orthodontic treatment help prevent cavities and periodontitis?
– Cavities and orthodontic treatment
According to the systematic review by Hafez et al., it is reported that crowding (misalignment) is not related to cavities.
Hafez HS,Shaarawy SM,AL-Sakiti AA,Mosta YA
Dental crowding as a caries risk factor: a systematic review.2012 Oct;142(4):443-50
http://www.ncbi.nlm.nih.gov/pubmed/22999666
– Periodontal disease and orthodontic treatment
In the systematic review by Bollen et al., there was no reliable evidence that treatment had a positive effect on the health of the periodontal tissue. There is no evidence to use for recommending treatment for preventing periodontitis to the large majority of patients.
Bollen AM1,Cunha-Cruz J,Bakko DW,Huaug GJ,Hujoel PP.J Am Dent Assoc. 2008 Apr;139(4):413-22.
http://www.ncbi.nlm.nih.gov/pubmed/18385025
In short, there is no scientific proof that connects orthodontic treatment with cavity or periodontitis prevention.
But we as dentists know clinically that there are cases where cavities and periodontitis partially progress due to crowding.
Even with no evidence, I do not feel it is wrong to suggest treatment to improve cleanability using a dentist’s discretion.
Also, it must also be remembered that cleanability and be negatively affected by the correction device.
There are cheek-side and tongue-side devices and also mouthpieces. Besides mouthpieces, all other devices must be worn for about 2 to 3 years, and cleanability is worsened.

This means that treatment does not suit patients with bad plaque control. I do, however, absolutely recommend treatment to improve cleanability to highly-motivated patients with good overall plaque control who cannot partially fix their crowding.

I also consider the patient’s cavity risks (pathogens, saliva) and periodontitis risks (pathogens). If the risks are great, crowded teeth can be a problem even with relatively good plaque control.
If performing treatment on patients already with periodontitis, there is quite the risk that it may progress further from the amount of corrective treatment and decline in cleanability. SPR or periodontal surgery must remove tartar beneath the gums, and plaque control fully implemented. Controlling any shifting that occurs after improving teeth alignment must also be taken into account.
First and foremost, after ensuring proper plaque control, decide the need for treatment.

3. Improving eating and chewing

This is the most simple. If patients have a hard time eating from their misaligned teeth and wish to improve it, it would be best to do treatment.
4. To prevent tooth loss due to force
Discussion for this is the most complicated.
When patients come to clinics themselves and ask for treatment, it is mostly to improve appearance. Dentists are the ones who recommend treatment to prevent tooth loss due to force. Dentists have a greater responsibility in their decision-making for this than for appearance.
It is possible to remove strong force with occlusal adjustment (slightly shaving the tooth) or a crown when the force is partial.
It is hard to prove that orthodontic treatment prevents tooth loss due to force, and mostly no scientific evidence as well.
is often used.
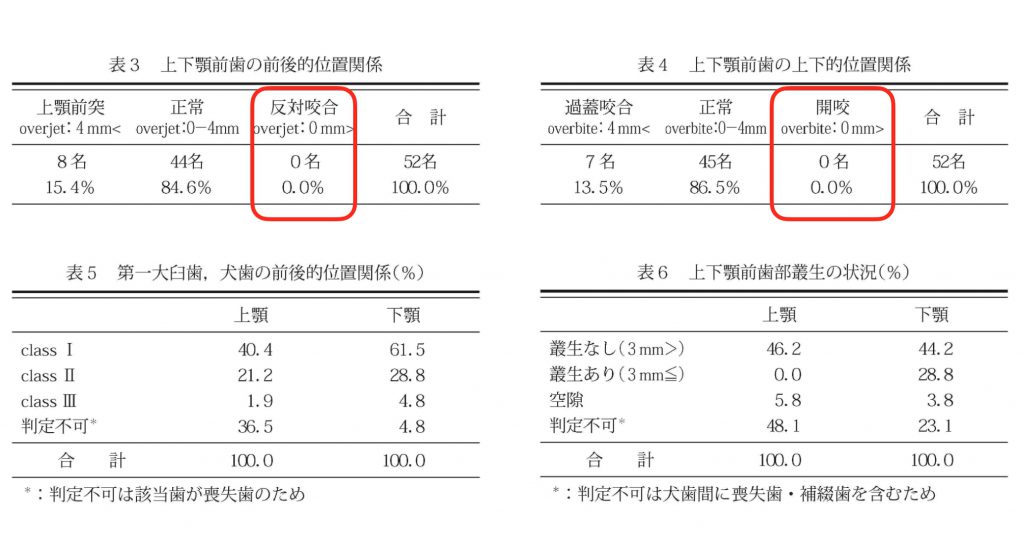
The occlusion of 52 individuals who has achieved the 8020 goal were investigated.
Among them,
84.6% had normal occlusion,
15.4% had maxillary protrusion (overbite),
13.5% had deep overbite (deep occlusion),
0% had reversed occlusion (protruding jaw),
and 0% had an open bite.
The results show that it is rather difficult to have 20 or more teeth over the age of 80 with a protruding jaw or an open bite.
Even the reference work “Observing the occlusion in elderly persons over 80 years old with at least 20 teeth”
shows similar results.
However, supposing we look at these figures, we could also assume that the number of people with reversed occlusion or an open bite were few to begin with. People with reversed occlusion is said to be 4 to 5%. From this, a result of 0% is not something that should cause fear. However, the fact is that there is still a significant difference. (Notwithstanding the sample size for both studies being a little small, with about 50 people)
Even then it is too quick to say that people with a protruding jaw or open mouth need treatment.
If thinking about affects due to strong force, you need to consider their force risks (degree of power). If you decide both the force and power is weak, the need for treatment is low.
I use a force risk diagnostic to investigate the risks of force.
There are greater risks with more prostheses. If natural teeth, there is acclimation due to the wear with enamel.
The basis of diagnosis is vague. It will be greatly influenced by the dentist’s learning environment, held knowledge, skills, and way of thinking.
For determining whether to treat patients orthodontically for occlusal reconstruction,
after considering the facial appearance and prosthetic space and determining the vertical dimension,
take the centric relation bite at that height, and mount the cast in the articulator.
Looking at the anterior coupling of the articular in this state, diagnose whether it is possible to address the problem with only a prosthesis.



When it is possible, if they already have a prosthesis on their maxillary anterior teeth, use only a prosthesis.
When they have many natural teeth, consider using composite resins or laminated veneers, then crowns. After thinking about the risks of grinding, consider treatment without dentures.
While treatment with a prosthesis carries risks such as shaving healthy teeth, damage or loss of teeth, and secondary decay, orthodontic treatment has risks such as time frame, cost, pain, and complications.
Because there are risks for orthodontic treatment and prostheses, I think it is best to use composite resins to address the problem in the least invasive manner.
Even if orthodontic treatment is unnecessary with an anterior coupling diagnosis, there are cases where it is better to have treatment for the facial appearance. In the end, it comes down to a comprehensive diagnosis.
5. Other (per opportunity)
When patients have several missing teeth, even if it is possible to just use implants, sometimes closing the spaces with full-jaw orthodontic treatment has a lower cost. This also improve the facial and intraoral appearance, killing two birds with one stone. Orthodontic treatment is sometimes recommended as the better alternative when looking at cost.
Although must evidence supports implants and they are a wonderful treatment, even they have risks. Scientific risks and not knowing if they will last 30 years. There are risks due to its artificial nature such as peri-implantitis, crown loss, and detachment. Natural teeth is always the best option if possible. Of course, there are risks with orthodontic treatment.
Comprehensively diagnose everything, explain it to the patient, and once you have gained their understanding, have them decide for themselves if they will undergo treatment.
I still have much to learn, but this was my summary of vital clinical points for considering whether orthodontic treatment is necessary for adults.

Thank you very much for reading until the end.
Please share this if you think it is useful.






関連記事 (Related Articles)


最近の投稿 (Latest Posts)
カテゴリー (Categories)
- マウスピース矯正(大阪/吹田) (103)
- インビザライン(大阪/吹田) (103)
- 歯ならび(大阪/吹田) (109)
- 見えない矯正(大阪/吹田) (103)
- 出っ歯の改善(大阪/吹田) (108)
- 八重歯の改善(大阪/吹田) (101)
- すきっ歯の改善(大阪/吹田) (99)
- 歯の矯正(大阪/吹田) (117)
- 矯正歯科(大阪/吹田) (108)
- 小児矯正(大阪/吹田) (101)
- 子どもの矯正(大阪/吹田) (101)
- CiAOアライナー矯正勉強会 (65)
- かみ合わせ(咬合)大阪/吹田 (132)
- i6(アイシックス)インプラント歯科勉強会/大阪 (36)
- インプラント(大阪/吹田) (90)
- 歯周病(大阪/吹田) (22)
- 根管治療(大阪/吹田) (3)
- お勧め記事 (TOPICS)大阪/吹田 (26)
- 予防歯科(大阪/吹田) (20)
- 審美歯科(大阪/吹田) (44)
- 歯科勉強会(大阪/吹田) (230)
- 歯科矯正日記(大阪/吹田) (1)
- 開業(大阪/吹田) (44)
- クリニック見学(大阪/吹田) (23)
- その他 (Others) (10)
- スペイン旅行 (8)
- 未分類 (2)
過去の投稿 (Past Posts)
- 2024年7月 (1)
- 2024年6月 (2)
- 2024年5月 (2)
- 2024年3月 (1)
- 2024年2月 (1)
- 2023年11月 (1)
- 2023年10月 (1)
- 2023年9月 (1)
- 2023年8月 (1)
- 2023年7月 (3)
- 2023年6月 (2)
- 2023年5月 (3)
- 2023年4月 (1)
- 2023年2月 (2)
- 2023年1月 (4)
- 2022年12月 (2)
- 2022年11月 (3)
- 2022年10月 (3)
- 2022年9月 (2)
- 2022年8月 (3)
- 2022年7月 (1)
- 2022年6月 (3)
- 2022年5月 (3)
- 2022年3月 (1)
- 2022年2月 (1)
- 2021年12月 (1)
- 2021年11月 (1)
- 2021年10月 (4)
- 2021年9月 (3)
- 2021年8月 (2)
- 2021年7月 (2)
- 2021年6月 (2)
- 2021年5月 (1)
- 2021年3月 (1)
- 2021年1月 (1)
- 2020年8月 (1)
- 2020年7月 (2)
- 2020年6月 (1)
- 2020年2月 (7)
- 2020年1月 (1)
- 2019年12月 (2)
- 2019年11月 (2)
- 2019年10月 (3)
- 2019年9月 (3)
- 2019年8月 (4)
- 2019年7月 (3)
- 2019年6月 (3)
- 2019年5月 (2)
- 2019年4月 (5)
- 2019年3月 (2)
- 2019年2月 (1)
- 2018年12月 (4)
- 2018年11月 (2)
- 2018年9月 (8)
- 2018年8月 (3)
- 2018年7月 (11)
- 2018年6月 (5)
- 2018年5月 (6)
- 2018年4月 (10)
- 2018年3月 (7)
- 2018年2月 (7)
- 2018年1月 (5)
- 2017年12月 (8)
- 2017年11月 (7)
- 2017年10月 (10)
- 2017年9月 (9)
- 2017年8月 (6)
- 2017年7月 (10)
- 2017年6月 (7)
- 2017年5月 (8)
- 2017年4月 (5)
- 2017年3月 (9)
- 2017年2月 (7)
- 2017年1月 (7)
- 2016年12月 (8)
- 2016年11月 (10)
- 2016年10月 (7)
- 2016年9月 (5)
- 2016年8月 (1)
- 2015年10月 (1)
- 2015年9月 (1)
- 2015年2月 (1)
- 2014年5月 (1)
プロフィール (Profile)

経歴
兵庫県洲本市出身(淡路島)
1997~ 2004年 神戸市消防局の消防士として従事
2005年4月 朝日大学歯学部入学
2011年4月 大阪歯科大学附属病院 口腔外科第1科臨床研修
2012年4月~2017年12月 医療法人幸恵会 カツベ歯科クリニック勤務 勝部義明先生に師事
2018年5月 こうつ歯科・矯正歯科開院
修了歯科勉強会
DAOアライナー矯正治療6daysコース修了(3期)(尾島賢治先生)
DAOアライナー矯正1dayセミナー修了(尾島賢治先生)
DSD(Digital Smile Design) 1dayセミナー京都(主催:DENTAL SQUARE JAPAN)修了
DSD(Digital Smile Design) 3days course Tokyo 2020修了(Dr.Christian Coachman・尾島賢治先生)
MAO(Molar-oriented Aligner Orthodontics)アライナー矯正3daysコース修了(有本博英先生・賀久浩生先生)
岡山矯正研修会Basic course修了(6期)(下間一洋先生)
岡山矯正研修会Advance course修了(5期)(下間一洋先生)
GPO(General Practitioner’s Orthodontics)アドバンス矯正コース修了(米澤大地先生)
GPO(General Practitioner’s Orthodontics)小児矯正コース修 了(米澤大地先生)
PDCセミナー(補綴と矯正の融合)修了(3期)(高井基普先生)
舌側矯正・インコグニート(Incognito Appliance System Certification Course)修了
マウスピース矯正(インビザライン)システム導入コース修了
混合歯列期の小児矯正歯科治療セミナー修了(保田好隆 先生)
プレオルソ小児矯正ベーシックコース修了(大塚淳先生)
PHIJ(Perio Health Institute Japan) ベーシックコース修了 (2019.5月~2020.1月)(築山鉄平先生)
PHIJ(Perio Health Institute Japan)カリオロジーコース修了(2019.12月~2020.5月)(安藤昌俊先生)
PHIJ(Perio Health Institute Japan)アップデートミーティング2020、2021参加
日吉歯科診療所オーラルフィジシャン育成セミナー修了 (2016.10月~2017.3月)(熊谷崇先生)
日吉歯科診療所オーラルフィジシャン育成セミナー修了 (2019.8月~2019.11月)(熊谷崇先生)
KDA(Katsube Dental Academy)Basic course修了(勝部義明先生)
KDA(Katsube Dental Academy)Advance course修了(勝部義 明先生)
咬合・補綴治療計画セミナー修了 (2016,5月~8月)(本多 正明先生)
大阪SJCDレギュラーコース2014年度修了(2014.4月~2015.2月) 第22期
大阪SJCDレギュラーコース2015年度修了(2015.4月~2016.2月) 第23期
大阪SJCDエンドコース修了
大阪SJCDマイクロエンドコース修了
ARDEC(Ariminum Research & Dental Education Center)Advanced Training into Research
Advanced Training Workshop On Periodontal Regeneration(Dr.Pierpaolo Cortellini、Prof.MaurizioTonetti)
大森塾3期生修了(大森有樹先生)
大森塾6期生修了(大森有樹先生)
大森塾ADPR(Academy of Dental Practice and Research)インプラント周囲の軟組織マネージメントコース修了
大森塾ADPR(Academy of Dental Practice and Research)インプラント定位置埋入・マイナーGBRコース修了
大森塾ADPR(Academy of Dental Practice and Research)TeCコース修了
韓国IMBD(International Meeting for Bonafide Dentistry)2015、2016、2017、2019参加
Total Solution JAPAN 京都坪井塾インプラント ハンズオントレーニング3ヶ月コース修了
i6 フィリピン共和国マニラ・バコロド インプラントトレーニングコース2016修了(中島康先生)
i6 フィリピン共和国マニラ・バコロド インプラントトレーニングコース2018修了
ストローマン・ジャパン主催Modified Block Bone Technique GBR ハンズオンセミナー修了
OSSTEMサイナスリフトマスターコース修了(洪性文先生)
JIADSペリオ6ヶ月コース修了(88期)
Maikai University & Asahi University School of Dentistry Continuing Dental Education咬合補綴コース修了(本多正明先生)
Maikai University & Asahi University School of Dentistry Continuing Dental Education サイナスリフトコース修了(嶋田淳先生)
Maikai University & Asahi University School of Dentistry Continuing Dental Education インプラント抜歯即時埋入コース修了(嶋田淳先生)
straumannインプラントオーバーデンチャーコース修了 (前田芳信先生)
石井歯内療法研修会セミナー修了(石井宏先生)
ivoclarダイレクトボンディングベーシックコース修了(天川由美子先生)
Ivoclarダイレクトボンディングマスターコース修了(高橋登先生)
kerrダイレクトボンディングコース修了(秋本尚武先生)
Forest-oneコンポジットレジン修復セミナー修了(岩田淳先生)
Biological Occlusion Seminar(Asami Tanaka,C.D.T ,President)
MiCD Practical Composite Restoration Basic Course修了(高橋登先生)
NPO法人 Japan Dental Mission会員(フィリピン共和国カオハガン島にて歯科医療のボランティア活動)
日本シミュレーション学会主催 セデーショントレーニングコース修了
所属学会・歯科勉強会
CiAO(Creative and innovative Aligner Orthodontics)アライナー矯正勉強会 代表
i6(アイシックス・インプラント勉強会)会員
日本顎咬合学会会員 認定医(咬み合わせ認定医)
日本矯正歯科学会会員
日本成人矯正歯科学会会員
日本IOBアライナー矯正歯科学会会員
インビザライン(マウスピース矯正)認定ドクター
日本アライナー矯正(マウスピース矯正)歯科研究会会員
日本口腔インプラント学会会員
STUDY GROUP N.H.K.所属
執筆
「 Healing at implants installed from ~ 70- to < 10-Ncm insertion torques: an experimental study in dogs 」
Oral and Maxillofacial Surgery. 2020 Jun 27. doi: 10.1007/s10006-020-00870-7.
「 Effect of lack of plaque control after the surgical treatment of peri-implantitis at surfaces with different characteristics: an experimental study in dogs.」
Oral and Maxillofacial Surgery. 2020 Jul 29. doi: 10.1007/s10006-020-00890-3.
「矯正治療とインプラント補綴を併用した咬合再構成症例」
DENTAL DIAMOND Feb 2020 VoL.45 No.661 P76-82
「強い咬合力に対応するために自家歯牙移植とインプラント 補綴を併用した咬合再構成」
歯科技工 June 2019 Vol.47 No.6 P536-548 共著
「インプラントを埋入した後で全顎的矯正治療を行なった咬合再構成(アナログ編)」
歯科技工 July 2019 Vol.47 No.7 P666-675 共著
「インプラントを埋入した後で全顎的矯正治療を行なった咬合再構成(デジタル編)」
歯科技工 August 2019 Vol.47 No.8 P772-784 共著
「診断用ワックスアップを活用した前歯部審美症例」
QDT Art & Practice May 2014 Volume39 No.5 P64-67
